For Investors & Payers
PainMAP solves a payer problem, not just a clinical one.
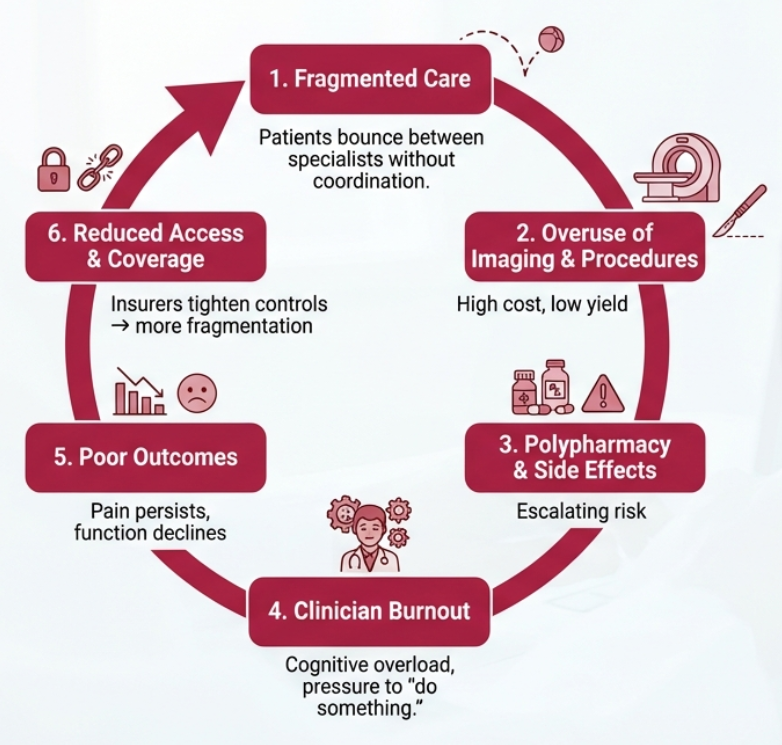
Chronic pain is one of the largest uncontrolled cost centers in healthcare. Fragmentation, unnecessary imaging, specialist overuse, and polypharmacy drive avoidable spend. PainMAP transforms chronic pain from a reactive cost center into a predictable, managed system.
Chronic pain: high cost, low precision.
- Chronic pain affects 1 in 5 adults.1
- Costs up to $635B annually.2
- Drives high rates of imaging, referrals, ED visits, and opioid prescribing.
- PCPs lack time and tools to perform mechanism-based assessments.
Payer impact: Chronic pain is a top driver of low-value care, unnecessary imaging, and high-cost downstream utilization.
National claims analysis3 reports ~$23.7M annual spend per 1,000 chronic pain patients. The spend is driven by:
$23.7M
Annual spend per 1,000 chronic pain patients.
The majority of this spend is avoidable. It accumulates through fragmented care decisions, overuse of imaging, trial-and-error referrals, and opioid-related downstream costs.
- Centers for Disease Control and Prevention. Chronic pain prevalence, United States.
- Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education. Relieving Pain in America, 2011.
- ISPOR 2022 national claims analysis.
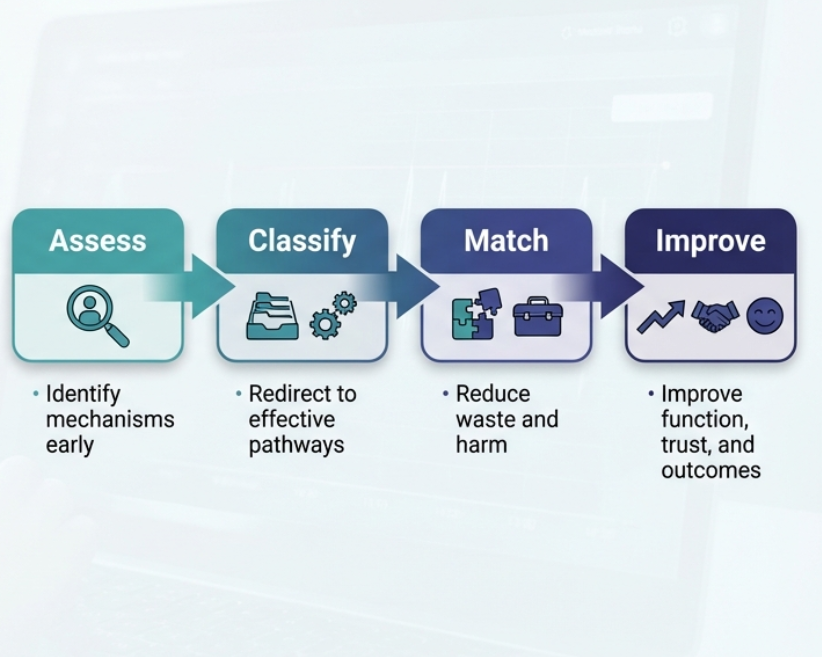
PainMAP: mechanism-based clinical decision support.
- Standardizes intake and mechanism classification
- Identifies red flags, safety risks, and opioid concerns
- Recommends guideline-concordant, first-line therapies
- Auto-generates payer-aligned documentation
- Reduces diagnostic wandering and low-value care
ROI outcomes expected.
Already validated by AHRQ, JAMA, BMJ, and other CDS precedents. Our validation pilots are in the pipeline.
- 20–30% reduction in low-value imaging
- 15–25% reduction in unnecessary referrals
- 2–5 minutes saved per PCP visit
- Lower opioid-related events and risk scores
- $450K–$900K annual savings per 100 PCPs
- ↑ PCP capacity and throughput
- ↑ functional outcomes for patients
Who will be early adopters of PainMAP.
ACOs / Risk-Bearing Groups
Direct financial incentive to reduce unnecessary utilization. PainMAP delivers measurable savings on one of the highest-cost patient populations.
Health Systems
Fee-for-service and value-based care hybrid models benefit from reduced imaging, fewer referrals, and faster visits without workflow disruption.
Employers / Payers
Chronic pain is a top driver of employee healthcare spend. PainMAP provides variance control in one of the most unpredictable cost categories.
ACOs / Risk-Bearing Groups
Direct financial incentive to reduce unnecessary utilization. PainMAP delivers measurable savings on one of the highest-cost patient populations.
Health Systems
Fee-for-service and value-based care hybrid models benefit from reduced imaging, fewer referrals, and faster visits without workflow disruption.
Employers / Payers
Chronic pain is a top driver of employee healthcare spend. PainMAP provides variance control in one of the most unpredictable cost categories.
Why payers and clinicians choose PainMAP.
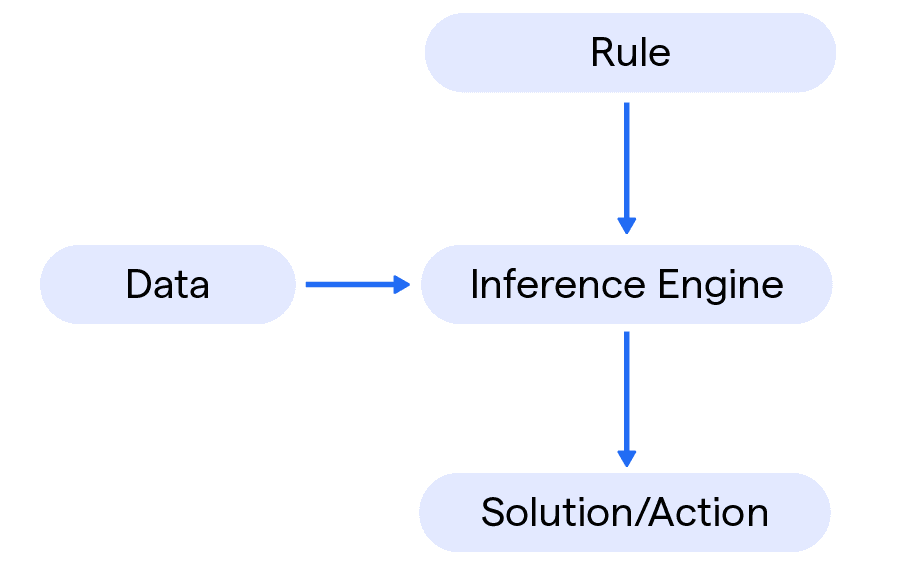
This is not another generic CDS tool. PainMAP addresses the root cause of waste: mismatched pathways leading to ineffective care. PainMAP is the first commercial system to extend the validated framework of CDS tools to chronic pain mechanisms, safety screening, and treatment matching.
01
Proprietary Mechanistic Model
Our pain classification engine is built on a proprietary model of chronic pain mechanisms. It goes beyond symptom-based guidelines to identify what is actually maintaining the condition, producing classifications that generic CDS tools cannot replicate.
02
FDA-Aligned Architecture
Every output is deterministic, traceable, and auditable. The system is designed from the ground up for regulatory alignment: no black-box predictions, no unexplainable recommendations. Each reasoning step maps back to patient data.
03
Therapy Matching + Safety Screening
PainMAP matches patients to targeted interventions based on mechanism, not trial-and-error. Built-in safety screening flags contraindications and low-value pathways before they are ordered. PCP-ready language supports payer justification.
04
Patient-Facing Expectation Setting
Patients receive clear, plain-language explanations of their pain drivers and care plan. This builds adherence, reduces frustration, and creates a shared understanding between clinician and patient that improves retention and outcomes.

Massive, underserved market
1 in 5 adults affected, and more than 57% are managed in primary care. We target early digital adopters in primary care — a scalable path to market share by capturing ~70% of that segment at an 8% penetration rate.
Clear payer value
Measurable cost reduction at the system level from day one.
Strong clinical need
Clinicians have no tools to classify pain mechanisms at point of care.
Defensible IP
Proprietary mechanistic model that improves beyond symptom-based guidelines.
Longitudinal data moat
Every assessment generates structured data that compounds our advantage.